Factors to Consider when using an AED
When treating a victim that has gone into cardiac arrest there are a few considerations to be made when it comes to using an AED (automated external defibrillator).
These considerations need to be made on
- Paediatric patients
- Wet or sweaty patients
- Patients with a hairy chest
- Patients with a medication patch
- Patients with a pacemaker or implantable defibrillator
If In doubt, start performing chest compressions and have someone contact emergency medical services via phone before you deliver an electric shock. If there are obvious signs of a cardiac arrest, acting fast will increase the patient’s chance of survival—no matter what other factors are present.
Treating a Paediatric Patient
Cardiac arrest in children is rare but still a possibility. Child patients require a reduced electrical shock if they are under eight years old or weigh less than 55 pounds. To cater to paediatric patients, some external defibrillators have a special paediatric setting, and others come with child electrode pads (either included with the device or sold separately).
For a child under age eight, adjusting an AED can be seen in example such as the below;
- HeartSine Samaritan PAD 350P. Unplug the adult electrode Pad-Pak and plug in the child electrode pads (sold separately). Follow the audio prompts and press the shock button when directed.
If no child pads are available, and your device doesn’t have a child setting, you can use standard adult pads. However, the chest placement is different for paediatric patients. One pad should be placed in the centre of the chest, and the other in the centre of the back. Use this placement for paediatric patients, whether you use adult or child pads.
See image below for reference;
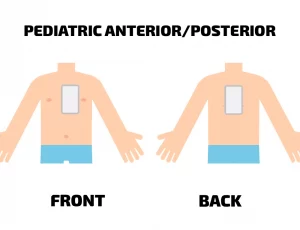
For an infant under 12 months, a manual defibrillator is more appropriate than an AED (automated defibrillator) —especially if no paediatric pads are available. However, it’s much better to use a portable defibrillator (with paediatric or adult pads) than to do nothing at all.
Treating a Sweaty or Water-Submerged Patient
Special considerations when using an AED with a patient also apply when the patient is wet or damp from sweat. Because water is an excellent conductor of electricity, the power of the shock would be dispersed across the patient’s body and be less effective where it’s needed the most.
When treating a victim of cardiac arrest who is wet or damp, remove them from the water (if they are immersed) and take them to a dry place. Dry off their chest area as much as possible and apply the electrode pads. There is no need to completely dry the patient from head to toe as time is of the essence, focus only on completely drying the chest area, specifically the area between the pads.
The most important factor is that the victim’s chest be dry so that the shock is delivered straight to the heart. If the victim is in a puddle or lying on a wet area of the floor but their chest is dry, simply move them away from the water and use the defibrillator as normal.
Treating a Patient with a Hairy Chest
When a cardiac arrest victim has excessive chest hair, it may be difficult for the electrode pad to analyse their heart rhythm and deliver an appropriately timed shock. This is because the hair would lift the pad up and off the patient’s chest, preventing full contact with the skin. The hair would also make it more difficult for the gel on the electrode pad to adhere to the skin.
There are three main solutions to the issue of chest hair, as recommended by the American Heart Association’s Basic Life Support Manual: BLS Provider Manual eBook (heart.org)
- Shave the hair off the area where the patch will be applied. It is sensible to keep a disposable razor stored with every AED specifically for this purpose. Most first-aid kids and first-responder kits should include at least one razor.
- If you don’t have a razor and the device continues to prompt you with “check pads,” push down hard on the electrode pads to increase conductivity. Then remove your hands when instructed to “stand clear.”
- If the machine still doesn’t respond, you can strip the pad quickly off the patient’s chest to remove some of the hair. Then apply a new set of pads. Only do this if you have extra pads on hand.
Treating a Patient with a Transdermal Medication Patch
Transdermal medication patches have been used since the 1970’s to deliver active medication, such as a hormone or nicotine, at a gradual rate through the skin. In the case of a cardiac arrest, medication patches present a burn hazard when using an external automated defibrillator if the shock is delivered over the patch.
Before applying an AED, remove the medication patch and wipe any sticky residue off the patient’s skin. It’s a good idea to wear gloves when removing the patch so that the medication is not absorbed through your skin.
Treating a Patient with a Pacemaker or Implantable Defibrillator
Pacemakers and implantable defibrillators make up the last category of special considerations when using an AED. If you place an AED directly over a pacemaker or defibrillator, the device may block the delivery of the shock. Instead, place the electrode pad a few inches lower or try an anterior-posterior (front-and-back) pad placement instead.
You can usually tell if a cardiac arrest victim has an implanted pacemaker or defibrillator because they will have a scar on either side of their upper chest or abdomen with a hard lump the size of a deck of playing cards or smaller. Most often this will be near the heart, on the left side of the chest, in which case it will not interfere with the standard pad placements. If they have suffered a sudden cardiac arrest, it’s almost certain that the device has stopped working. Don’t worry about damaging the device as this can be replaced.
Conclusion
With a few simple adjustments, you can use an automated external defibrillator on the patients mentioned above, as you would on any other. Make sure your AED is equipped with paediatric pads, a razor, and a pair of gloves and you should be ready for anything.
Special Considerations When Using an AED Device (aedleader.com)








